

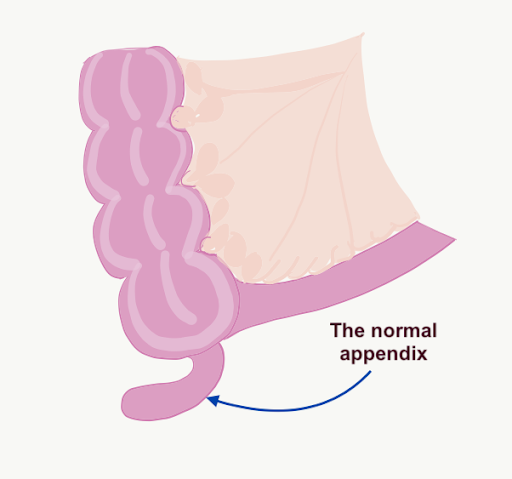
The normal appendix
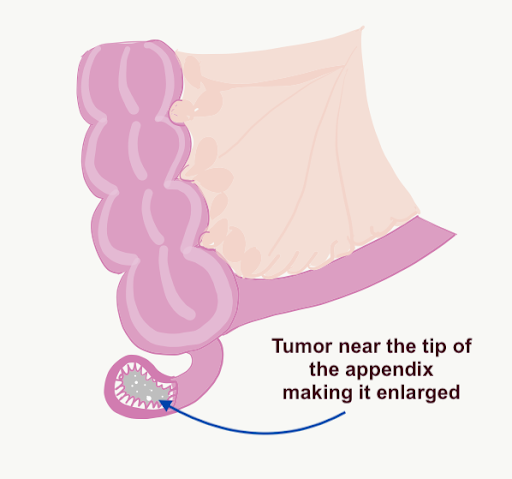
Mucinous tumor in the appendix leading to swelling of the appendix
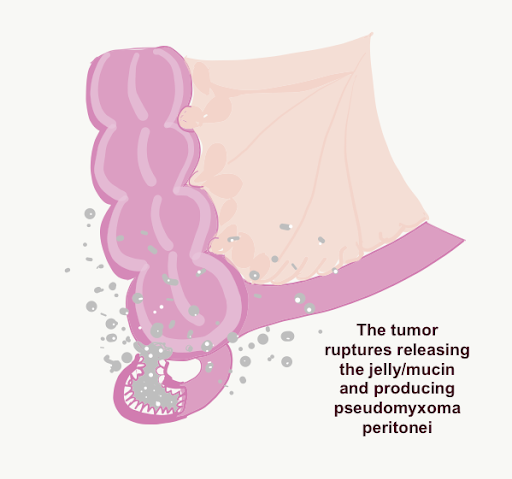
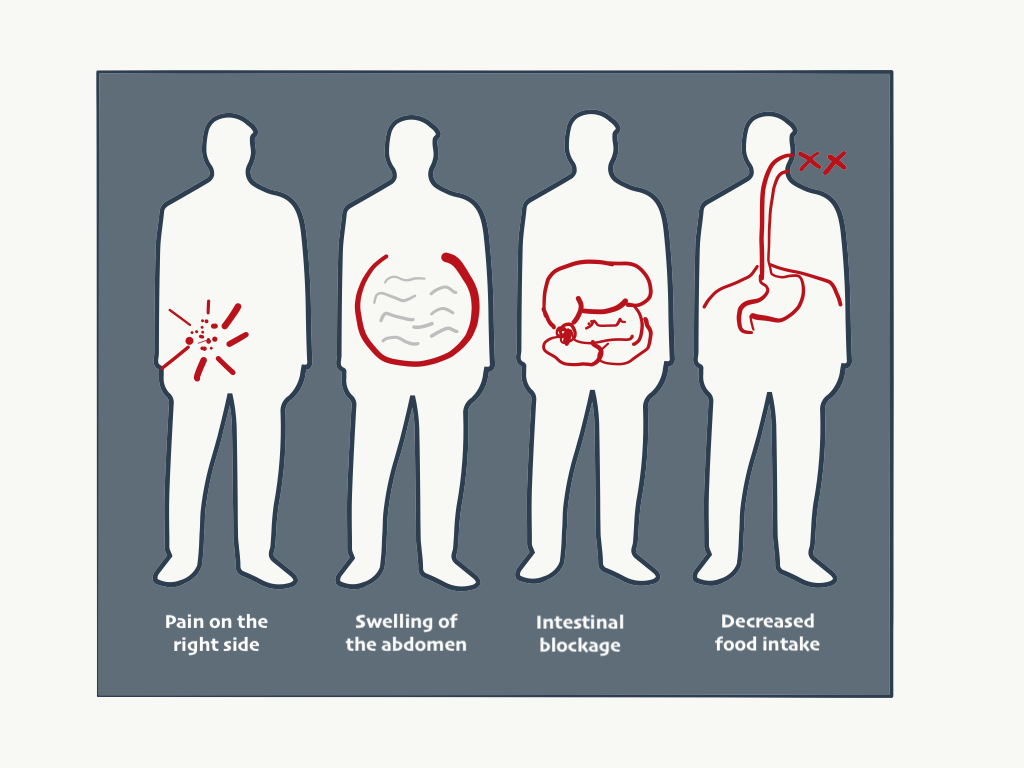
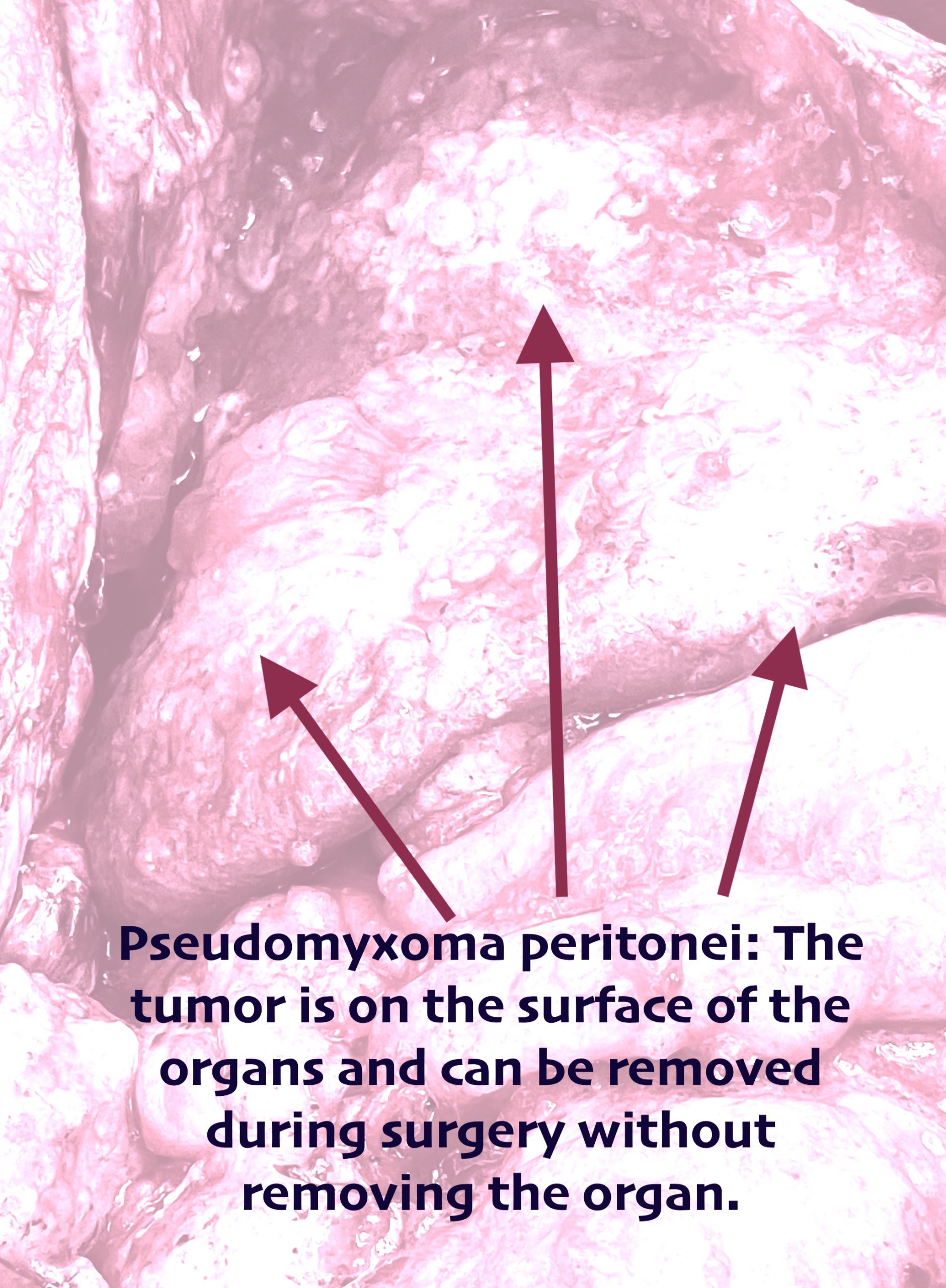
The appendix ruptures and releases the mucinous tumor which implants all over the peritoneal cavity resulting in pseudomyxoma peritonei or jelly belly

The normal appendix
Mucinous tumor in the appendix leading to swelling of the appendix
The appendix ruptures and releases the mucinous tumor which implants all over the peritoneal cavity resulting in pseudomyxoma peritonei or jelly belly