
Peritoneal Cancer Spread from Colorectal Cancer
Colorectal cancer is the second most common cause of peritoneal cancer spread of all the
gastrointestinal cancers
Know about
Know about Colorectal Cancer
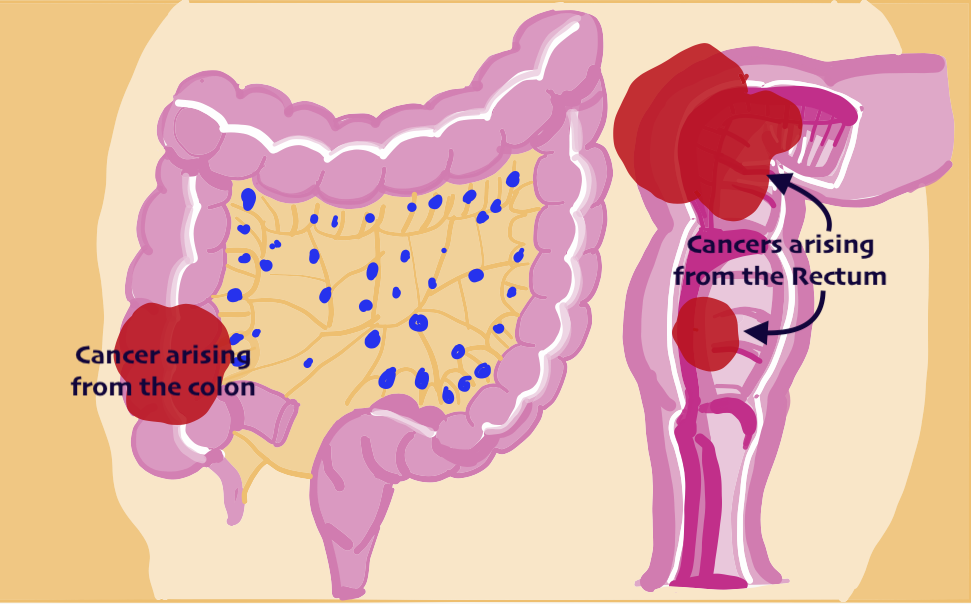
Colorectal cancer originates in the colon or the rectum. The colon is the part of the digestive system where the waste material is formed. And the rectum is the end of the colon adjacent to the anus which stores waste material. Together, they form a long, muscular tube called the large intestine (large bowel).
Tumors of the colon and rectum are growths arising from the inner wall of the large intestine. These cancers are also known as colon cancer and rectal cancer.
Together they are known as ‘colorectal cancer’.
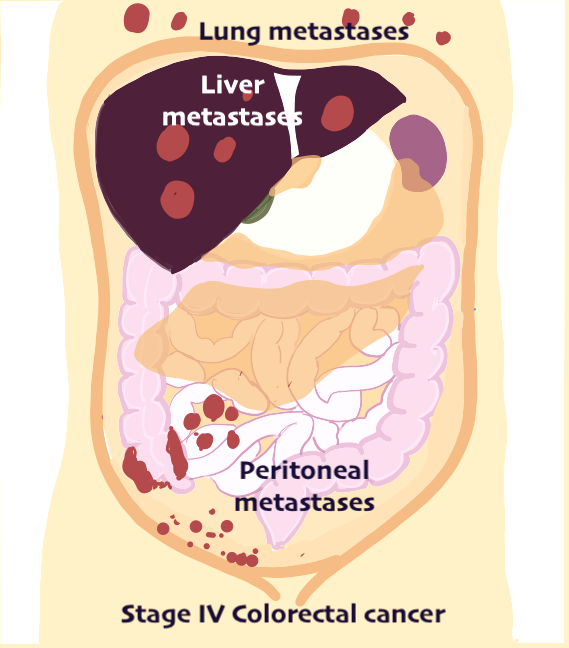
Stage 4 Colorectal Cancer
When a cancer arising from the colon or rectum spreads to other organs like the liver, the lungs, the peritoneum , distant glands, it is known as stage 4 colorectal cancer.

What is Colorectal PM
Presence of cancer in the peritoneum in colorectal cancer is known as Colorectal PM or colorectal peritoneal metastases. In colorectal cancer , peritoneal cancer will develop in about 15-20% of the patients.
Colorectal PM may be found along with the primary tumor (synchronous colorectal PM) or months or years after the primary cancer has been treated (metachronous colorectal PM). Patients with advanced tumors that have involved all the layers of the wall of colon (T3 and T4 tumors), tumor that cause blockage of the intestine, or a perforation (hole in the intestine), tumors that have spread to the lymph nodes or that have spread to the ovaries are at a higher risk of developing peritoneal cancer spread compared to patients with tumors that do not have any of these features.
Treatment of Colorectal PM
There are three important components of treatment of colorectal PM: Cytoreductive surgery, HIPEC and Systemic (intravenous chemotherapy).
All three components of treatment are essential for good long term results. Some patients may get systemic chemotherapy first followed by cytoreductive surgery and HIPEC or vice versa in others.
It is very important to know the extent of disease in colorectal cancer while treating it.
A PET CT scan or CT scan may be done to see:
Spread to other organs
Patients with peritoneal implants often have seeding in the liver or lungs. In 5-10% of all patients however, seeding is limited to the peritoneum. It is for this subgroup of patients cytoreductive surgery and HIPEC may be an option. In some selected patients with 1-3 tumors in the liver or lungs and peritoneal cancer, surgery could still be possible.
Extent of spread in the peritoneal cavity
It is important to know the extent of spread of the tumor in the peritoneal cavity. The surgeon measures the amount of cancer in 13 different regions of the abdomen and gives each region a score from 1 to 3. These scores are added to a global score (Sugarbaker’s Peritoneal Cancer Index).
In colorectal PC a PCI score of >20 indicates that surgery and HIPEC may not be useful. These patients are treated with systemic chemotherapy alone. In patients who have a very good response, surgery and HIPEC may be attempted. However, recent scientific evidence has shown that even some of the patients with a high PCI can benefit from cytoreductive surgery and HIPEC. The score also tells us about the prognosis. The less the score, the better the outcome.
Complete tumor removal from the peritoneal cavity
The most important factor is complete tumor removal. If the surgeon can completely remove the tumor from all regions of the abdominal cavity, the surgery will be more beneficial. If the surgeon is unable to completely remove the tumor from all regions, surgery is not undertaken.
